Click on each step or next arrow to view content
1RPE65 gene delivery
2RPE65 protein production
3Restoring the visual cycle
1RPE65 gene delivery
RPE65 gene delivery
RPE65 gene delivery
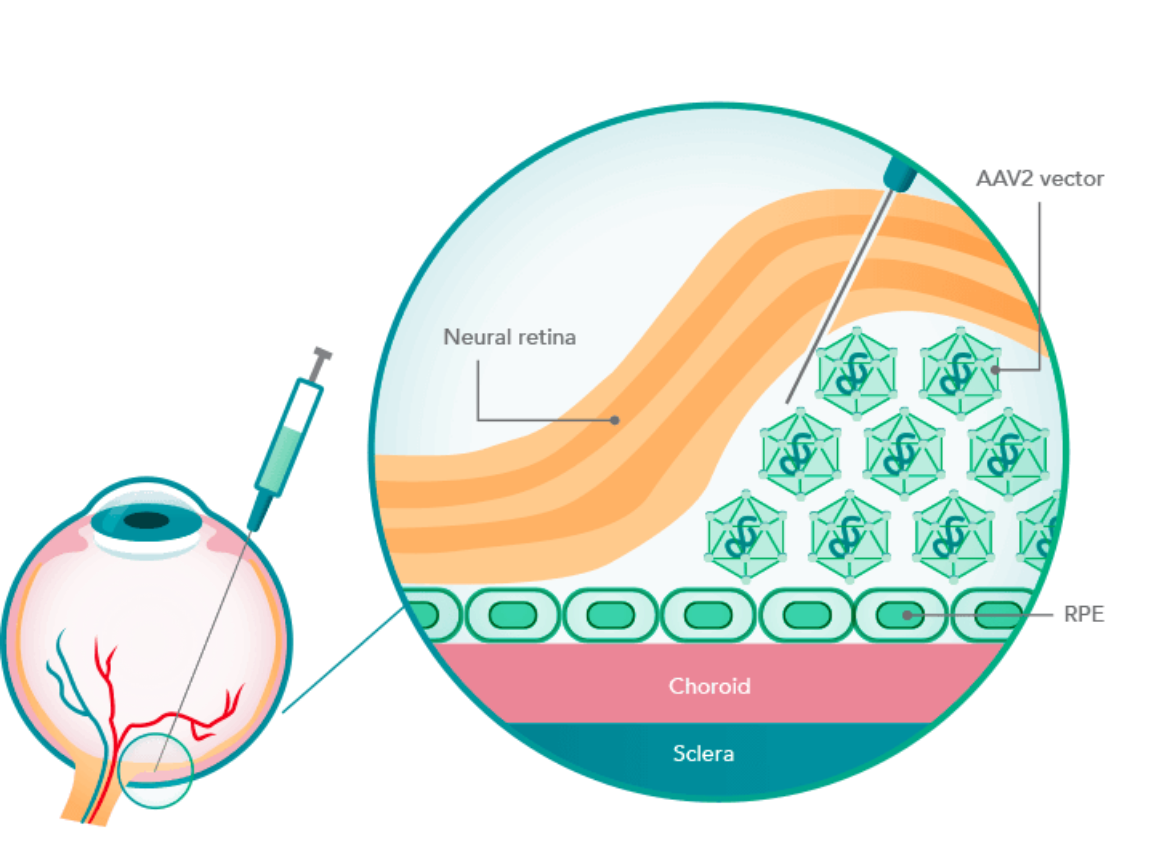
LUXTURNA uses the adeno-associated viral vector serotype 2 (AAV2) to carry a functional copy of the RPE65 gene into the retinal pigment epithelial (RPE) cells to compensate for the RPE65 mutation.2-4
2RPE65 protein production
RPE65 protein production
RPE65 protein production
With a functioning RPE65 gene, the cells begin producing the RPE65 protein.2,5


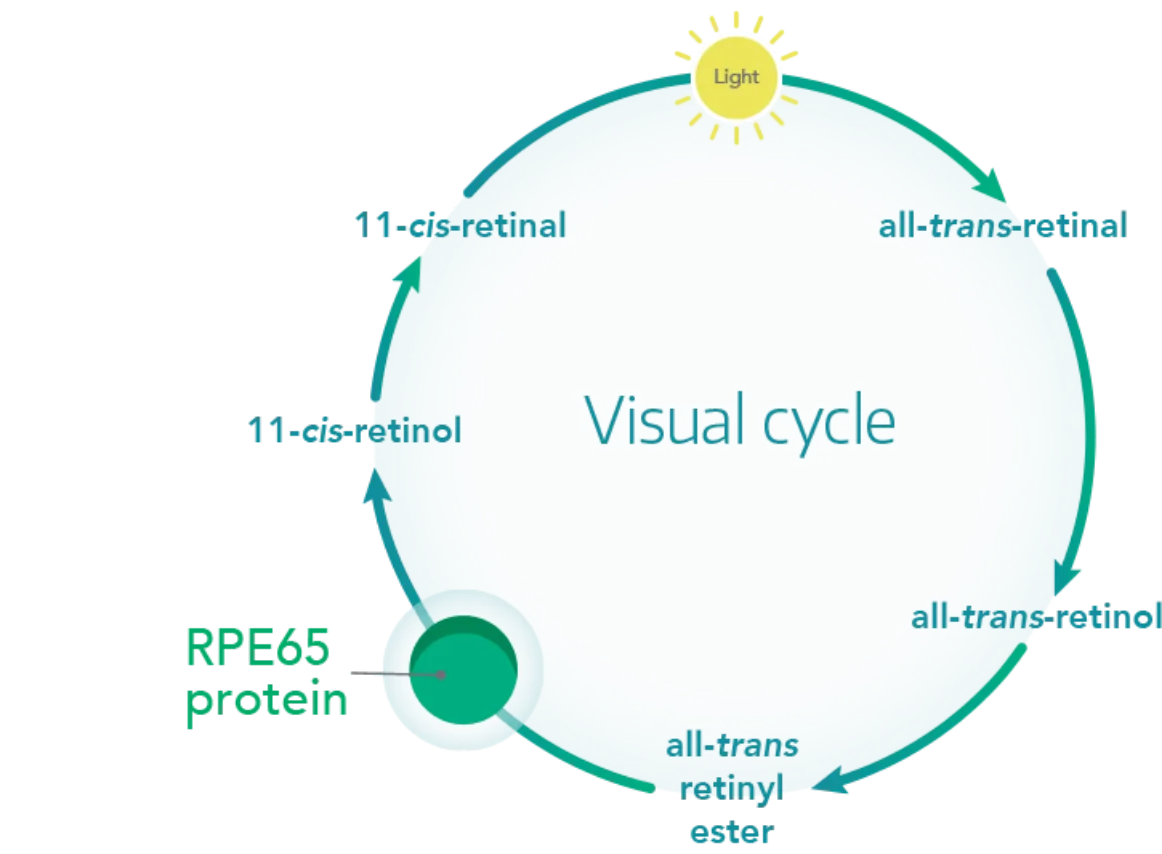
3Restoring the visual cycle
Restoring the visual cycle
Restoring the visual cycle
With the functional RPE65 protein, 11-cis-retinal (a critical visual pigment component) regenerates to restore the visual cycle.2,6